Shoulder X-ray의 Anatomy와 Positioning
1. Basic view
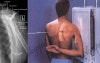
1) AP view
Helpful for: Glenohumeral Arthritis, Coracoid Process Fracture, Glenoid Fracture, Proximal Humerus Fracture. Posterior Glenohumeral Instability.
Evaluate: humeral head postion relative to glenoid; AC joint position/arthritis; RTC calcifications, acromial spurring
Acromiohumeral interval: normal = 7-14mm. <7mm indicates Massive RTC Tear. (Weiner DS, JBJS 1970;52B:524). May appear falsely decreased with posterior subluxation of the humeral head.
Position: Patient erect, turned 30-35° toward the side being xrayed
Tube: Perpendicular to plate

2) Axial view : Superio-inferior, Inferio-superior


2. Special view
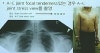
1) Lateral view(=Scapular “Y” view, Trans-scapular view)
Demonstrates: lateral projection of scapular body and humeral head overlapping the glenoid.
Helpful for: Shoulder Dislocation, Proximal Humerus Fracture, Scapula Fracture
Position: Erect with anterior aspect of affected shoulder against x-ray plate and rotating other shoulder out 40 deg°.
Beam aimed from posteriorly along scapular spine
2) Neer view(=Supraspinatus Outlet view)
Demonstrates: outlet/impingement of the supraspinatus and coracoacromial arch.
Helpful for: Subacromial Impingement, assessing Subacromial Morphology, unfused acromial epiphysis.
Position: Erect with anterior aspect of affected shoulder against x-ray plate and rotating other shoulder out 40 deg°.
Beam: aimed from posteriorly along scapular spine but with the beam aimed with 10° caudal tilt

- Axillary view
Demonstrates: glenohumeral joint narrowing (best view), Os Acromionale, glenoid version, glenoid erosion, humeral head subluxation.
Helpful for: determining the amount of acromion which remains in patients who have undergone previous surgery; relation of humeral head to glenoid; Hill-Sachs lesions, Os Acromionale, Acromioclavicular Arthritis, Shoulder Dislocation.
Position: Patient seated at side of radiographic table with the arm abducted and axilla over the cassette. Beam: angle 5°-10° toward the elbow, central beam directed at the shoulder joint.
Many alternative postions for similar xray, can be supine etc.

4) West point axillary view
Demostrates: anteroinferior glenoid rim., best for osseous Bankart Lesion.
Helpful for: Shoulder Instability, Glenoid Fracture, osseous Bankart Lesion.
Postion: Patient prone with affected shoulder resting on a pad @8cm for the table top. Casette positioned against the superior apsect of the shoulder.
Beam: aimed 25° from horizontal (to tables surface) and 25° medially (to patients midline).

5) External & Internal rotation view
① External rotation view
Helpful for: Glenohumeral Arthritis, Coracoid Process Fracture, Glenoid Fracture, Proximal Humerus Fracture, compression fracture of humeral head.
Position: Patient erect, turned 30-35° toward the side being xrayed; arm maximally externally rotated
Tube: Perpendicular to plate
(Blue dot = Greater Tuberosity, Red dot = Lesser Tuberosity)

② Internal rotation view
Helpful for: Hill-Sachs lesions, Glenohumeral Arthritis, Coracoid Process Fracture, Glenoid Fracture, Proximal Humerus Fracture.
Position: Patient erect, turned 30-35° toward the side being xrayed; arm maximally internally rotated
Beam: aimed perpendicular to plate
(Blue dot = Greater Tuberosity, Red dot = Lesser Tuberosity)

6) Stryker’s view
Demonstrates: humeral head
Helpful for: Hill-Sachs lesions (best view), Bankart Lesion.
Position: Patient supine with cassette posterior to the shoulder. The hand placed on top of the head. The elbow should point straight upward.
Beam: directed 10° superiorly/toward the head, centered over the coracoid process. (Hall RH, JBJS 1959;41-A:489-94)

3. Acromioclavicular joint
1) AP view(Zanca view)
Demonstrates: AC joint and distal clavicle
Helpful for: Acromioclavicular Arthritis, Acromioclavicular Joint Separations, Distal Clavicle Osteolysis, Distal Clavicle Fracture
AC joint spurring and cystic changes indicates Acromioclavicular Arthritis.
Distal clavicle elevation indicates Acromioclavicular Joint Separations.
Position: Erected with cassette behind shoulder. Beam:Xray beam aimed at the AC joint in 10° to 15° cephalic tilt. Xray penetration should be 1/2 normal to avoid overpenetration of AC joint.

2) Weighted(stress) view
- Sternoclavicular joint
* Serendipity View
Demonstrates: sternoclavicular joints and medial 1/3 of the clavicles.
Helpful for: Clavicle Fracture, Distal Clavicle Fracture, Sternoclavicular Joint Dislocation.
Postion: supine with cassette under upper chest
Beam aimed at clavicle or manubrium (SC pathology) with a 40° cephalic tilt.
